

Even When They Look Good on Paper... The dental industry has spent years perfecting the blueprint. The problem was never the blueprint. It was assuming the blueprint would hld on its own.
...But They're Not the Solution Either. The debate over AI call handling is missing the point. The question was never whether to answer more calls — it's whether your practice can hold the patients who come through them.
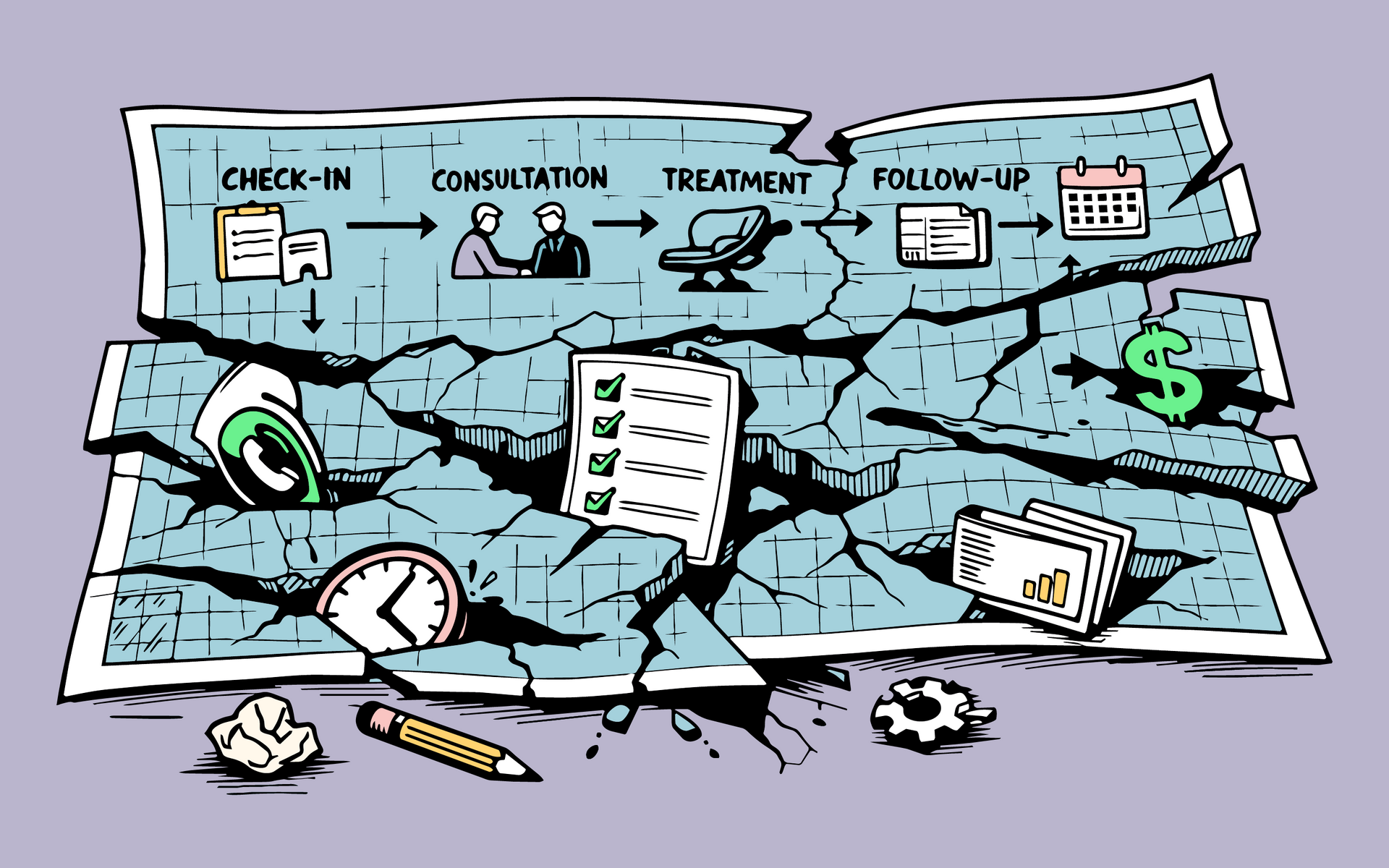
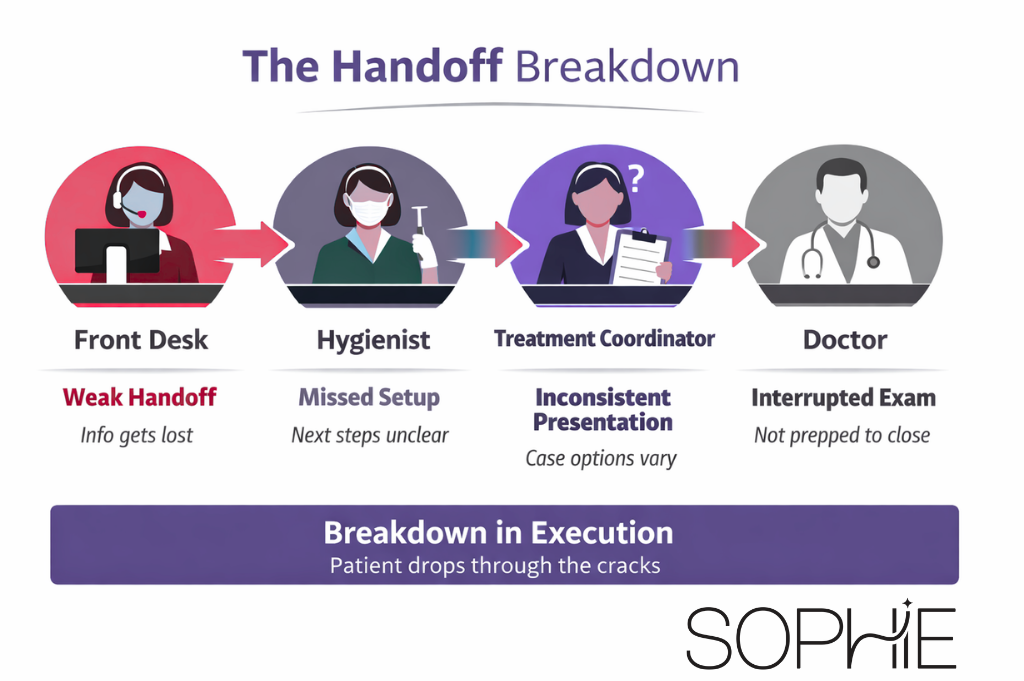
Your Process Isn't the Problem. Your Execution Is. Most dental practices already know what to do. The gap isn't knowledge — it's the system that makes sure it actually gets done. Walk into almost any dental practice today and you'll find a recognizable structure. Scheduling, check-in, consultation, diagnosis, treatment, follow-up. The stages are mapped. Roles are assigned. Metrics are on someone's dashboard. And yet, two practices running what looks like an identical operation will produce wildly different results month after month. That inconsistency rarely comes from a broken process. It comes from something harder to fix: the gap between a defined process and a performed one. The Map Is Not The Territory On paper, the patient journey is sequential and controlled. In reality, it's full of places where execution quietly falls apart. A call gets missed and nobody loops back. A treatment plan gets presented once, then dropped. A follow-up sits in a task list until it doesn't. A financial conversation loses momentum and the case goes cold. None of these are training failures. The staff knows what should happen. The breakdown is in the handoff between knowing and doing — and it compounds silently until it shows up in your numbers.

Most small to midsize dental practices don’t have a growth problem. They have operational leaks costing $100K–$300K+ per year. Learn why visibility doesn’t fix it and how to measure what actually holds.

Most dental practice software tracks activity—but doesn’t ensure execution. Learn why case acceptance, unscheduled treatment, and insurance aging persist—and what actually fixes it.

If your dental practice improves—but never stays consistent—this explains why. Discover the hidden reason execution keeps breaking (and what actually fixes it).

Dental consultants drive improvement—but why doesn’t it last? Discover the real reason change fades and what’s missing inside dental practice operations.
You trained your team. So why isn’t the work happening consistently? The real reason training fails in dental practices—and what actually fixes it.

Task tools are built for projects—not real-time clinical operations. Here’s why they break in dental practices and what actually works instead.

Your reports show exactly what’s wrong—but nothing changes. Here’s why dental analytics tools fail to improve performance.
